SLP Chat
This will be a place where therapists can share ideas, problem solve and express concerns. Lets work together to make our jobs easier!
Teresa
Speech Language Pathology Gifts?

Did you know that Amazon carries a variety of Speech Therapy gifts/Speech Language Pathology gifts. I guess if you went to ASHA you might have seen some of these odd little trinkets. Some are rather cute and some are a little freaky. I love my job but you would have to live a Speech Language Pathology lifestyle to use some of them. I could put links to over 229 items. I’m just going to pick out a few for fun.
“What the he-double hockey sticks is it?” People will be afraid to ask
A little creepy
My tree felt empty without this
This will leave the other guys asking, “Where can I get one?”
If I want to keep the kids and my husband away from my car, I’ll put this on it
Doesn’t Advanced Health Care usually give this stuff away?
Think I could use this to carry my wine to school?
This is rather cute but should it be Speech Language Pathologist instead?
I just hope my family doesn’t find this page on Amazon. If they did I could only imagine my birthday and Christmas gifts for the rest of my life. Come to think of it we use to get my Mother all kinds of nursing trinkets. What were we thinking?
How SLPs can deal with Middle School rudeness

I received a question from a middle school therapist asking if I had any suggestions on how to deal with rude disrespectful students. No other information than that in terms of community, severity of students, size of groups or gender. From my 15 plus years of experience at the middle school level I think I relate to the situation she might be in. I’m going to assume her students are mainly boys and basically language/learning disabled students.
Three things to consider. First, Speech Language Pathologists do not also have to be experts in behavior. We have enough on our plate. Second, the rules have changed just in the past few years and we are not always allowed to use our professional judgement on who will continue to benefit from therapy and who will not. Third, middle schoolers specialize in rudeness, but it shouldn’t be consistent.
As few as 5 years ago I was able to go into a middle school annual review meeting, explain any behavioral difficulties that might be going on. I would proceed to tell the parent that the student isn’t working in therapy and not really getting anything out of it. Parents usually realized the issue because they were dealing with similar behaviors or complaints at home. We kept any language accommodations and modifications in place but the student was officially discharged from therapy. These days students have to “test out” of therapy before they can be discharged. We all know that “testing out” rarely happens for our language kids. Hence our professional judgement is ignored by the system. However, at least at a 3 year reevaluation you can bring up concerns around not continuing to benefit from services.
They are middle school aged children and figure if they keep behaving badly they eventually won’t have to go to therapy. Keep in mind that these children are probably having considerable difficulty in middle school as the language demands in all subjects quickly becomes more difficult. Going to therapy isn’t cool. I’ve been fortunate to work in schools for the past 20 or so years that have been on the cutting edge of integration services. Most kids accept each other and do not pay much attention to the limitations of typical language/learning disabled students. You might want to consider your schools history in terms of special education integration.
I use to be able to tempt the students with food treats once in a while. However, that was before all the food rules schools now have. A granola bar, cookies, dum dum pops or a stick of gum went a long way. By feeding them it showed I cared. It was something special to look forward to and most middle schoolers are hungry all the time.
Some middle school students that were embarrassed to be in speech therapy, especially if someone had the bight idea for me to see them in the classroom. Rudeness could be the result of embarrassment.
If you think you students are embarrassed about having to go to therapy here are some suggestions.
- Talk to them about therapy, what they are working on, who made the decision that they would have to see you (yes include parents), try to do pull out therapy whenever possible. Polling my middle school students over the years, few wanted me breathing down their necks, in the classroom with their friends watching.
- Spend time working gently on raising awareness of their language needs
- Don’t label your door if you don’t have to. If you do just put your name.
- I think all therapy rooms should have windows in their doors but make the student’s seat placement outside the view of the window so their friends don’t see them.
- Explain any scheduling decisions
- Don’t show up at the classroom door to pick them up, make a phone call to class instead.
Here are some other suggestions you might try
- If the groups aren’t working try changing them up (I realize that is easier said than done because our scheduling is based on the school schedule). Are your groups too big to manage?
- Try changing your therapy methods to make activities more fun. Throw in a game once in a while, even if it is a game that has little to no educational value.
- Laugh with your students. I created a joke curriculum that focused on many aspects of ambiguous and figurative language along with vocabulary.
- Occasionally give them a day off, especially if there is something going on in class that they want to be part of. Cut session short once in awhile, they like that. (this of course depends how strict your administration is on comp services)
- Be firm, make it clear that you are tired of their rudeness. It’s ok to use your mean teacher voice when necessary. Follow up with an activity that they like then thank them for their cooperation or tell them this was a fun group.
- Occasionally bring in classwork and let them finish homework, help them muddle through a book they’re reading.
- Design some activities where they can get up and move around. A white board comes in very handy for this.
If these suggestions don’t have any effect, its time to bring your issues to the principal or vice principal. It might be a good issue to pose to teachers at staff meeting. Teachers and counsellors might be able to provide some insight or even support. At the very least you’ll find out if this is a general school issue or individual specific. More than likely these kids are rude everywhere not just in therapy.
As mentioned earlier middle schoolers specialize in rudeness. Our language disabled students have difficulty knowing when it might be ok to be rude and when it isn’t. Most middle schoolers will not be blatantly rude to adults other than their parents but it does happen. Keep in mind they’re a bundle full of hormones and sometimes can’t help it. Rudeness shouldn’t happen on a consistent basis. If you see a problem try talking privately to the student about it or if you know there are issues mention it to the guidance counsellors/school psychologists.
Middle School Therapists, please feel free to add any additional suggestions
Good Luck
Professional Liability for SLPs

Outside Evaluations-Are they really that specialized anymore?

As a school speech language pathologist, I haven’t been impressed with outside speech and language evaluations for quite awhile. What I’ve noticed over the past several years, from the outside evaluations that have landed on my desk is that not one has been in-depth or used a variety of unique tests to aid differential diagnosis. The general format for these outside evaluations is now the CELF (Clinical Evaluation of Language Fundamentals) and maybe the PPVT (Peabody Picture Vocabulary Test). The reality is that most school speech language pathologist probable give the CELF more often and are just as good at interpreting the results. Most of the time after reading an outside speech and language evaluation, I have more questions than concrete information. Very few outside evaluations go the extra mile these days. I usually end up finding the language information contained in neuropsychological reports more comprehensive and helpful.
When I first started working in the mid-80ies my school assessments were not as detailed as they are today. Perhaps we could chalk that up to a lack of experience but I think was just the way things were done. Back then we usually recommended that more involved students go out of school and obtain a comprehensive evaluation involving several disciplines. Where I lived many of the hospitals provided comprehensive evaluations focusing on child development and academics.
Those outside evaluations often included physicians, developmental specialists, educational specialists, psychologists, physical therapists, occupational therapists and of course speech language pathologists (then referred to as speech therapists by most). What made these teams special was that they took the time to meet with the children over several sessions then met as a team to compare findings after that presented evaluations and service recommendations to parents. While those evaluations were detailed, the one problem was that those evaluations teams rarely looked beyond the clinical setting. Schools then received findings and recommendations, weeks if not months later. Schools were rarely included in the actual process or the final meetings.
Reading those evaluations was always an education in itself. The speech language pathologist’s report was usually peppered with tests I had only seen in grad school or not at all. It was learning experience to read and compare findings from all disciplines especially the medical and neuropsychological side. Most of the time I felt those comprehensive evaluations were in-depth, provided a key to the students learning style and provided specific information to aid differential diagnosis.
While those evaluations gave us a good insight into the child’s learning style and needs, the outside evaluations often lacked the knowledge on how to design therapy approaches that could actually be implemented in a school setting. I remember the speech and language therapy recommendations (along with most other disciplines recommendations) were often too grand to be carried out in the public school setting. The outside evaluations gave us some very good information but these highly specialized teams had little understanding on how to realistically service students in the public school setting.
Since those days, laws have changed. Schools were made financially responsible for almost all testing. Special education evaluation services in schools had to evolve. Everyone involved in special education had to know how to diagnosis without having the clout to diagnosis.
Schools were now purchasing test material that were cutting edge. Speech language pathologists, special educators and school psychologists were learning how to assess students and look deeper into a child’s overall needs. Schools began offer a greater variety of services and outside evaluation recommendations became fewer and fewer. The school evaluation process became not only more comprehensive but more of a team effort.
While I liked the information obtained through those outside comprehensive evaluations, the way we do it now is better. We know the students we’re testing, we have a feeling on how they will do in the curriculum, we can recommend services that fit the school schedule, suggest services that are best suited to the child and work as a team with the parents. If we need or want a true “diagnosis” we will send students out for neuropsychological evaluations or other specialized testing.
In the past clinical speech language pathologists (and their teams) had the inside track on assessing language issues in school aged children but I don’t feel that is even close to being true these days. Our school assessments have become so specialized that school evaluations teams often know exactly what is going on with a student before testing begins, we are able to consult on what areas to target, talk to teachers about current performance and observe the child in the school setting. Many schools are able to purchase some of the evaluation tools needed to dig a little deeper. However, budget constraints and time factors will keep many school evaluators from being up to date and cutting edge. There is still a place for outside evaluations but clinical speech language pathologists who claim to be evaluation specialists need to step their game and differentiate their approach.
Outside evaluators need to keep in mind the reason why the students come to them in the first place. It’s not always because of schools doing a poor job. Schools may need your expertise or just be limited terms of materials. Outside evaluators from all disciplines should consult with the school professionals, as a courtesy, to review previous work with the student, ask about areas of concern and find starting points for extended testing. Clinical speech language pathologists, please don’t send school speech language pathologists reports containing just the CELF-5 or another similar common test battery without consulting us. Find testing tools that will enhance test results not repeat results. Please keep in mind that sometimes we need your strong but flexible recommendations to support our findings. Be aware of the constraints of the school day. Special education students have a lot of issues to deal with and there are only so many hours in the day. Please do not sent the same recommendations for every student you evaluate, it only lessens the impact of your recommendations.
With our more challenging cases we often want and need outside input. Find ways to make your findings and recommendations meaningful and helpful
This is the third of three (long winded:) articles focusing on the School Speech Language Pathologist and the problems with their changing role. This really goes against what is trending in education. My first two articles “Have School Speech Therapists Lost Their Focus” and “Is the gap widening between school speech language pathologists and clinical speech language pathologists” generated a lot of interest. As always looking for you feedback.
Professional Liability for SLPs
Q-Global Survey
Hi Everyone,
I’m still looking for a few more SLP to complete the Q-Global survey I put up earlier this month. Right now it looks like most of you are not using it, trusting it or can afford it. I’ve worked with Q-Global and they have responded to our needs. However, I am really disappointed with Pearson. Like they will ever care.
If you have a few minutes to fill out the survey please follow the link to my original article. https://theschoolspeechtherapist.com/survey-q-global-and-the-celf-5/
Thanks in advance
Teresa Sadowski
Professional Liability for SLPs
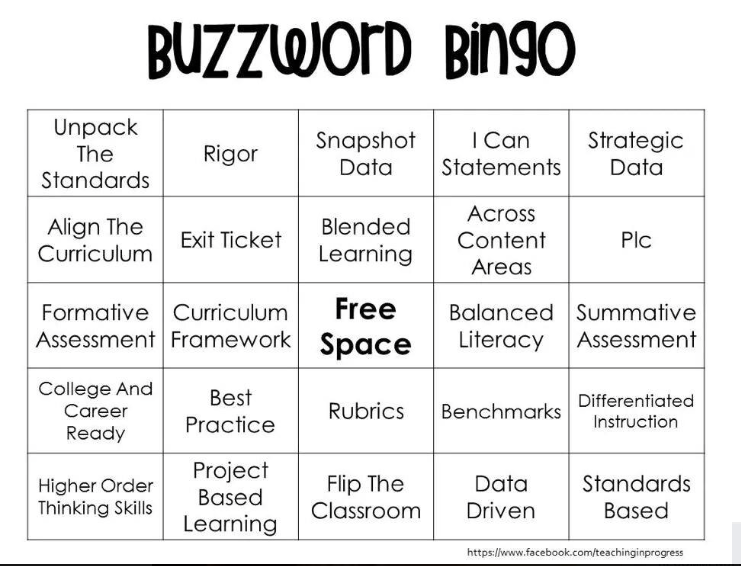
Have a good chuckle but think while you’re laughing
A few weeks ago I saw this “Buzz Word Bingo Card” floating around Facebook. So much of this buzz word bingo had to do with measuring what students have learned rather than how/what students are being taught. I assumed that that was why it made it on some of the funny education and anti-common core pages. Does any buzz word here actually tell you anything about what the students are learning? I’ll let you generate your own opinion on that. Now compare this buzz word bingo card to the one below.
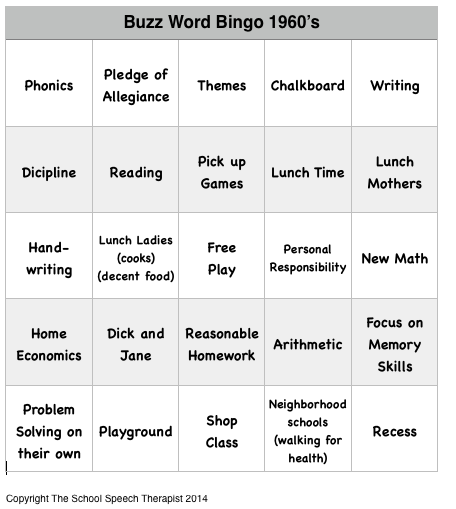
Here is the Buzz Word Bingo that teachers might have shared in the late 1960’s. Granted someone would have had to recreate it and run it off on on mimeograph machine (which were still used until the early 80ies). It is important to note that using the Buzz Words from the 1960’s, many children received a good solid foundational education. Was it perfect? No. Was awareness yet heightened around learning and language disabilities? NO! However, the good teachers who did not have bulging classrooms did try their best to help all children succeed. I know there was more teaching and less measuring. I know many of you may have hated Dick and Jane but guess what the formula worked for a variety of children, giving them not only reading success but self confidence to read. My favorite three on the Buzz Word Bingo 1960 are PHONICS, HANDWRITING and FOCUS ON MEMORY SKILLS.
Thanksgiving Humor

I found these Thanksgiving themed jokes floating around Facebook this week. Even though it’s after Thanksgiving I am going to use these (or some of these) in therapy this week. I believe they’re still relevant because the students just experienced Thanksgiving and with any luck remembered some of the details. I am big on teaching how to recognize and understand humor. Understanding humor is a huge part of social pragmatics. I often have an objective focusing on humor written into my student’s ed plans.
If students can’t “get it” they are often left behind both within the social realm and as curriculum/materials becomes more challenging. Subtleties in language are all around us, from tv to textbooks. Some kids “get it” easily and naturally and some do not. Most of our language disabled kids need a lot of help learning how to “get it”.
15 Thanksgiving Jokes
- What happened when the turkey got into a fight?
He got the stuffing knocked out of him. - What did the baby corn say to the mama corn?
Where’s the popcorn? - Why did the police arrest the turkey?
He was suspected of fowl play. - What are unhappy cranberries called?
Blue Berries. - What sound does a turkey phone make?
Wing! Wing! - What kind of car would a pilgrim drive?
A Plymouth. - What is a turkey’s favorite dessert?
A Peach Gobbler. - When does Christmas come before Thanksgiving?
In the dictionary! - How does a turkey drink her wine?
With a gobble-let. - Why did the cranberries turn red?
Because they saw the turkey dressing. - What do turkeys use to clean themselves?
A feather duster. - Why did the pie go to the dentist?
Because it needed a filling. - What kind of music did pilgrims listen to at the first Thanksgiving?
Plymouth Rock - Why do potatoes make good detectives?
They keep their eyes peeled. - How many cooks does it take to stuff a turkey?
One, but you really have to squeeze him in.
Originally compiled by Michelle Regna BuzzFeed Staff
http://www.buzzfeed.com/michelleregna/15-thanksgiving-jokes-your-grandma-will-eat-up
Professional Liability Insurance for SLPs
Shopping on Amazon this Season

With Cyber Monday beginning for some probably today, if you order from Amazon remember to order through your favorite blog (such as mine) Look for the Amazon link on the site and order from there. Or sign up for Amazon smile and send a few pennies to your favorite charity. It truly is only pennies but every little bit adds up. Since I can’t order through my own blog, I support the Trustees of Reservations.
Survey: Q-Global and the CELF-5
Last January I wrote a couple of articles about Pearson’s Q-Global scoring system. As result had some nice conversations with Pearson regarding the scoring for the CELF-5 and how we use the data. In response to my concerns and the concerns of many other SLP’s, Pearson made some nice changes to the Q-Global system.
Q-Global Scoring and the CELF-5
This week I ran into a new challenge with Q-Global, I had to purchase some scoring credits. My school system does not have an account. I assume my colleagues are scoring by hand and without complaint since I haven’t heard anything. I wanted to buy 10 scoring credits. Pearson’s web site made this difficult to do quickly. I ended up having to spend time calling Pearson only to be told the credits would not be available for one to two hours. Which for such a big company in this day and age was unacceptable. Of course I sent this concern to my contact at Pearson.
Then I started wondering, just how many SLP’s are actually using the Q-Global system on a regular basis. I’m curious but not sure I would get a straight response from Pearson. So I put together a short survey asking some simple question to try and figure out if SLPs are using Q-Global on a regular basis and if SLPs like it.
CELF-5 and the Q-Global Survey
Is the gap widening between School Speech Language Pathologists and Clinical Speech Language Pathologists?
Reading articles and comments on my blog I’ve begun asking myself what I think are a couple of key questions. Is the gap widening between the school speech therapist and the clinical/hospital therapist? Why don’t we function the same way? Actually I’ve been thinking of this for a long time ever since an administrator, in passing at a staff meeting said something like, “They have to realize this is a public school”, in reference to a parent who wanted extra services in the ideal setting. At the time I thought privately to myself, why wouldn’t you want us providing the best services possible on parr with clinical or private therapists.
So do school Speech Language Pathologists and Clinical Speech Language Pathologists function the same way? I know the answer to that would be no. So my next question is why don’t speech language pathologists working with the same types of students all function the same way? School SLPs should be clinicians first and focused on curriculum based services second, after the student has achieved skills at a certain level within the therapy setting.
Why can’t school SLPs provide the same intensive services as a therapist working in a clinic? The first obstacle to this is scheduling. With some creativity and flexibility with administration and teachers I do believe this could be overcome. However, the reality is that test prep and curriculum has almost taken away the ability to be flexible with student’s time. We as therapists would also have to convince schools that intensive services would possible yield a better outcome and hopefully get the students out of therapy sooner. Honestly this is where I fell push in therapy really misses the mark. The second obstacle is staffing. In most (I dare say all) school systems therapists are spread so thin that intensive services are almost impossible to provide. How did school speech language pathologists get to the point where caseloads are so large they can’t be flexible.
When I started thinking about the differences in how school aged children are serviced by the SLP at school and the SLP working in clinical setting I raised more questions than I expected. I think time on task is almost less important of an issue when compared to how goals are written an addressed. However, my one haunting question is why, if our training and purpose is supposed to be the same, why are students serviced so differently in these settings?
SLPs working in the clinical setting have the flexibility to look at speech and language issues from a developmental perspective and address specific needs. Clinical therapists can also write goals that are meaningful and can be measured informally through task performance/observation. While clinical therapists may consider curriculum and homework when designing therapy, they are not asked to focus only on certain threads within a curriculum. School therapists are now being asked to design goals that are related to curriculum rather than looking at the developmental needs of the child. Our training tells us that if children do not develop skills in a prescribed manner, splinter skills are likely to emerge. Given the nature of the students we service, they are already at very high risk of developing splinter skills, why would we support that. School therapists are asked to service students within the classroom setting occasionally taking on the role of co-teacher. In theory, co-teaching might look like a good model on paper but some students may still require intensive services to make progress.
The college curriculum focused on the clinical model as most speech and language programs still do today. SLP’s are trained to have specific understanding of language development, linguistics, overall child development including reading. We’re trained to evaluate and work with students who have different learning styles and disabilities of all types that effect language development and learning. We learn how the brain works. Nowhere in my training was it ever mentioned that I had to water down my role as a language specialist to take on classroom responsibilities. (**In the right setting and with the right population co-teaching/classroom consultation can work but it is not a cure all to manage language disabilities or a large caseload)
So why are we as school SLP’s willing to push aside our clinical training to service students in a manner that focuses on curriculum rather than child development. Water down our therapy and time on task almost forcing (the more astute parent) to look for private services. Letting the private clinical therapist look like they are better trained and know more than we do? Why aren’t we servicing our students in the manner we were trained? These are some questions to ponder as our role in the schools evolves and changes. It’s my opinion that school SLPs need to be more in control of how students are serviced given the limitations of the public school setting rather than being dictated to by administration, common core curriculum and mandated test prep.
So why shouldn’t school SLPs function in a similar manner to clinical or private practice SLP? Sure there are going to be some differences because of the different settings. Have the restrictions become so great on the school SLP that they cannon function in the best possible manner? Has the gap become so large between the school SLP and the clinical SLP that school SLPs do not look or feel as competent? What do you think?
This is the second of three articles focusing on the School Speech Language Pathologist and the problems with their changing role. This really goes against what is trending in education. My first article “Have School Speech Therapists Lost Their Focus” generated a lot of interest. As always looking for you feedback.
Have school Speech Language Pathologists lost their focus?
When I went to school my courses focused primarily on child development, language acquisition, understanding how the brain worked (and didn’t work), remediation techniques for articulation and language and learning about disabilities that resulted in a language delay or impairment. We didn’t just learn about working with kids or adults but all ages and disabilities. My coursework was clearly based on a medical model but I was trained to work in all settings.
Throughout my career, I’ve carefully evaluated my students, identified their strengths and weaknesses through testing designed specifically to assess language functioning across receptive, expressive and pragmatic areas. Based on my testing, I wrote goals that focused on improving “language” abilities. I always felt that my purpose was to target and improve underlying language skills. The goal was to improve language abilities so students could be on the path to develop mature adult language, function among their peers, work independently, do well in school, have a shot at successful higher education and become productive adults.
At what point did the role of the Speech Language Pathologist change within the public schools? Who was it that thought it would be good for the Speech Language Pathologist to base their goals on the curriculum rather than the child’s development or skill level? Several years back in one school system I worked for, it was made very clear to me that we were not supposed to be thinking in the “medical model”. I found that just absurd since language and learning are brain based. My vast experience also told me that if students did not acquire language in a prescribed developmental manner gaps in language development, understanding and usage, would be the end result.
The way we are supposed to provide “therapy” and write goals has changed, yet our testing and most of our materials have remained the same. That’s a clue right there. The materials we use are rarely leveled. We use our clinical judgement to find appropriate starting points, when to raise/lower the bar and when modification of instruction/material is needed. Language develops on a continuum, ideally developing and improving slowly over time. Language skills are extremely difficult to measure on a weekly basis. With any luck at all you are raising the level of the material slowly but how can that really be reflected in the goal?
I know I sound like an old therapist who can’t accept change. Perhaps maybe that’s part of it. However, I also know that children need strong underlying language abilities to “access the curriculum” (I am so sick of that term). Writing our goals and changing our methods to reflect specific curriculum will not target underlying skills, no matter how you spin it. It’s my belief that working on language through curriculum only promotes the development of splinter skills. We are therapists not co-teachers. That doesn’t mean that I am not familiar with school curriculums or that I don’t occasionally incorporate a vocabulary list, book or specific classroom task into therapy. Reality is school Speech Language Pathologists only see students 1-2 times a week, hardly enough time to keep up with specific classwork. Therapy groups may consist of students from different grades/classes. That alone makes working within curriculum on a regular basis impossible. (I do realize there are other effective therapy models that are designed to work within the curriculum but those SLP’s are not carrying 50+ students on a caseload and those schools are supporting time for program development.)
My feeling is schools do not realize what skills Speech Language Pathologists bring to the table. They don’t understand how extensive and varied our training was. Note that School Psychologists (who also base their training on a medical model) have not been asked to change in the same way Speech Language Pathologists have. Because we are trained in the medical model we have a deeper understanding of why students have language/learning disabilities. We know how to help remediate language using specific techniques/materials unrelated to school curriculum. We need to reclaim our role as “therapists” in the public schools. Given the changes that have taken place in education, I’m not sure that’s possible.